8.1.4.7
3030 – Participant Health Summary
Print and give this to each family as part of their transition packet when they are transitioning out of our program at any time during the year.
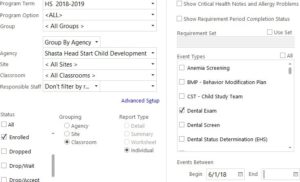
Program Term: “Your Program” (EHS/FCC/HS) and current program year
Agency: Shasta Head Start Child Development or EHS-CC Partnership
Site: “Your Site”
Classroom: “Your Classroom” (if you have multiple classrooms, see “Advanced Setup”)
Status: Enrolled Group: Classroom
Event Types: Check only the following:
Dental Exam (HS Only)
Dental Screen (EHS/FCC Only)
HealthHist HDNA
Hearing Hemoglobin/Hematocrit
IHP-SHS Individual Health
Lead
Medication
Physical/WBC
Tuberculosis
Vision
Events Between: Begin: “Start of Program Year”
End: “Last Day of enrollment”
Always Preview your report before Printing.